



Ureteroscopic LithotripsyUreteroscopic lithotripsy of lower ureteral calculi may reduce the necessity of open surgery. Compared with ESWL, its advantage lies in higher rate of stone evacuation. As reported, ureteroscopic treatment of lower ureteral calculi is 96%-97%. For long-existing stones, ureteral adhesion and even polyps may be present, which is hard to eliminate with ESWL but can be solved effectively with calculus forceps in ureteroscopy. Ureteral "stone steps" formed after ESWL can also be solved by ureteroscopy. Reports in China document the incidence of complications of lower ureteral calculi to be 2%-8%, mainly consisting of injuries to the ureter such as perforation and laceration, hematuria and ureteral constricture. All of these complications can occur due to unskillful practices. There were 6 cases (3.3%) of ureter perforation and 4 cases (2.2%) of ureteral constriction in the URSL group. Thus, ureteroscopy strictly demands gentle operation techniques and clear view of the calculi in order to avoid ureteral injury. If ureteral perforation or laceration is found, a double J tube needs to be indwelled for one week. 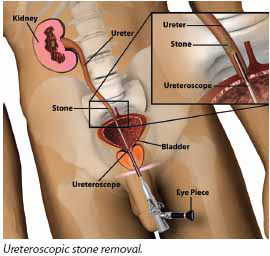
TUUL (URETEROSCOPIC STONE REMOVAL) Stones in the lower ureter (the tube connecting kidney and bladder) can be treated by ESWL or Ureteroscopy or Laparoscopy. ESWL has a high failure rate for lower ureteric stones, as the bony pelvis within which the ureter lies will absorb some energy of the shock waves. Laparoscopy is a procedure reserved for some difficult stones, were open surgery is anticipated. The normal ureter is about 3-4mm in diameter. A ureteroscope is a highly specialized telescope that can be passed into the ureter via your bladder to visualize the stone on a video screen. The ureteroscope we have is a very modern instrument with a diameter of only 2.3mm diameter. This is then connected to a TV screen enabling x10 to x15 magnification. Through the ureteroscope, we can pass probes to powder the stone. The large fragments are then removed by graspers for stone analysis. You may be requested by the doctor to sieve your urine after the procedure to collect stone fragments for analysis. A small 2mm stent (internal tube) may have to be left inside, extending from the bladder to the kidney, depending on type of stone being treated. The stent allows for quick recovery of the kidney and better healing of the ureter. It occasionally causes pain while passing urine and occasional blood stained urine. The stent will not be seen outside the body and can be removed any time between a month and 3 months or earlier if the bladder irritation is intolerable. Removal of the stent does not require admission. Sometimes, when the ureter is too narrow or when the stone is too impacted, ureteroscopic removal of the stone is done in 2 stages. In the first stage, a stent alone is inserted and in the second stage the stone is removed. ROUTINE PRE OPERATIVE CHECK If possible this is completed before admission or on the morning of admission, if no medical problems are anticipated. ADMISSION You should come for admission to the Urology department OP on the date of admission. Admission is usually fixed the day before surgery. PRE OPERATIVE CHECK If possible this is completed before admission or on the morning of admission, if no medical problems are anticipated. 1.Routine pre-operative check up will be done by me, the physician and the anesthetist, if this has not been already done. If you have any preference regarding General or Spinal Anesthesia, inform me and discuss it with the Anesthetist. 2.Preparation for surgery will be done in the evening and will involve shaving of private parts and an enema and fasting for more than 4-6 hours before surgery. 3. The time of surgery will be informed today. DAY OF SURGERY 1. There may be a delay of about an hour if the theatre is not ready. 2. You will have a catheter (tube) through your water passage in to your bladder. This will be maintained for one day to decrease pain from the water passage. 3. You will be in the intensive care postoperative room for about 4 hours. 1st POST OPERATIVE DAY 1. The catheter would be removed the next day morning. 2. 24 hours bed rest is required after Spinal Anaesthesia. Light diet is advised. 3. You may be requested to sieve your urine to collect fragments for analysis. Sieve is available in the hospital pharmacy. 4.You should maintain a urine output of at least 2.5L /day requiring you to drink a glass of fluid every hour, except when you are sleeping. 6. Normally you will be allowed to go home.
|
+91 - 95661 39630
+91 - 94441 68963