



LAPARASCOPIC ADRENALECTOMYThree different surgical approaches have been described for laparoscopic adrenalectomy, including the transabdominal lateral flank approach, anterior transabdominal approach, and retroperitoneal approach. Although each technique has its merits and proponents, the transabdominal lateral flank approach is most often used and is discussed here Port positioning and laparoscopic access Laparoscopic access may be obtained by an open or closed technique based on surgeon preference and expertise. The authors' preference is to place a Veress needle just below the costal margin and pre-insufflate the abdominal cavity. This is followed by optical trocar entry with a 5-mm trocar at the midclavicular line, approximately 2 finger breadths below the costal margin. This 5-mm trocar can be later "upsized" to an 11-mm trocar. An alternative is an open cutdown at this area; however, the incision needed for this usually requires the placement of a 10-mm to 12-mm trocar or balloon-type trocar to prevent leakage of pneumoperitoneum. Four laparoscopic ports placed in the right subcostal region are typically required for laparoscopic right adrenalectomy, although some reports on the single-incision techniques have recently emerged. Port positioning and size of ports vary and are surgeon dependant. However, at least one 11-mm to 12-mm port is required for clip applier or endoscopic stapler accommodation. The remainder of the ports may be 5-mm ports. Our typical port placement involves a 10 -mm to 12-mm trocar placed in the subcostal region at the anterior axillary line (camera port), a 10-mm to 12-mm trocar in the subcostal region at the midclavicular line (surgeon's right hand working port), a 5-mm trocar in the subcostal region just to the right of the umbilicus (liver retraction), and a 5-mm trocar in the posterior axillary line subcostally (surgeon's left hand working port; see the images below). 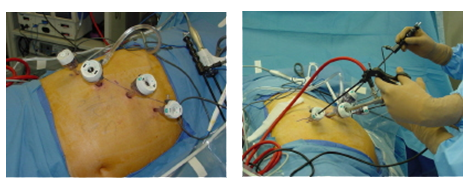
Port positioning for laparoscopic right adrenalectomy Port positioning for laparoscopic right adrenalectomy. Alternatively, the surgeon can use the 2 "inside" ports for working ports and have the camera coming in from the port in the posterior axillary line. |
+91 - 95661 39630
+91 - 94441 68963